After childbirth, mothers’ pelvic floor muscles often sustain varying degrees of damage. It’s recommended to test your pelvic floor muscles during postpartum checkups to understand how far they’re from normal function and what kind of treatment and recovery plan you need. Today, we’ll look at pelvic floor muscle testing methods and painless pelvic floor rehabilitation exercises every rehabilitation therapist should know!
Overview of pelvic floor muscle function
Ⅰ Dissection
Superficial layer : ischiocavernosus muscle (clitoral erection); bulbocavernosus muscle (tightens the vaginal opening and clitoral erection); superficial transverse perineal muscle (repairs the perineal body); external anal sphincter (closes the anal canal and helps with defecation)
Middle layer : Deep transverse perineal muscle (compresses the abdominal wall of the urethra and vagina, supports the perineal body and vaginal opening)
Deep layer : Levator ani (the main muscle of the pelvic floor, helping to close the rectum); coccygeus (flexes the tailbone)
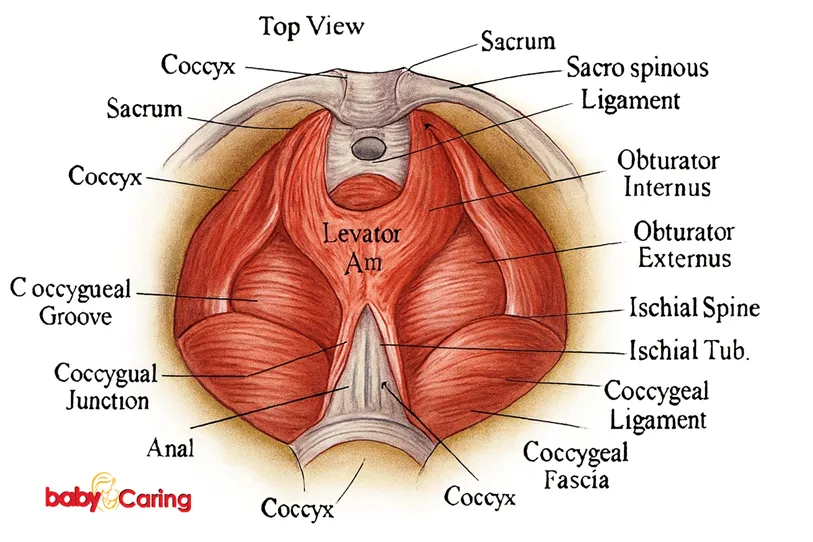
The levator ani muscles are the most important supporting structure of the pelvic floor. Based on their fiber origins, insertions, and arrangement, they are divided, from anterior to posterior, into the pubovaginal, puborectalis, pubococcygeus, and iliococcygeus muscles. The coccygeus muscles, located posterior to the levator ani muscles, are paired, weak, triangular muscles interwoven with tendon fibers. The pubovaginal muscles, the primary sphincter of the female vagina, are called the pubovaginal muscles. When the pubovaginal muscles are tense and spasmodic, they can cause dyspareunia; when they are weak, vaginal laxity occurs.
II. Pelvic floor muscle fiber classification and function
Type I (slow-twitch) fibers are associated with maintaining resting support, are long-lasting and continuous isometric contractions, and are not prone to fatigue. These fibers comprise over 70% of the deep pelvic floor muscles.
Type II (fast-twitch) fibers are associated with the rapid and powerful contraction of the pelvic floor muscles. They are isotonic, quick and concise, and easily fatigued. They play an important role in maintaining sexual pleasure.
III. Main causes of pelvic floor injuries
1) Pregnancy and childbirth injuries;
2) Increased abdominal pressure, such as chronic constipation, coughing, sneezing, prolonged weight-bearing and other exercises that increase abdominal pressure;
3) Congenital abnormal development of pelvic floor muscle collagen fibers;
4) Aging and ovarian dysfunction lead to decreased estrogen secretion, which weakens and loosens the pelvic floor support tissue;
5) Malnutrition. Severe nutritional deficiency can lead to muscle atrophy, relaxation of the pelvic fascia, and loss of support for the uterus, vagina, and urethra.
2 pelvic floor muscle screening methods
Ⅰ POP-Q score
The POP-Q scoring system can more accurately assess the degree of pelvic organ prolapse and is currently the most authoritative evaluation system for pelvic organ prolapse. The positioning and significance of POP-Q reference points:
Using the hymen as a reference (point 0), six points on the anterior, posterior, and apical sides of the vagina (two points Aa and Ba on the anterior wall, two points Ap and Bp on the posterior wall, and two points C and D on the apical side) and the total vaginal length (tvl) are used as scales to quantify prolapse. The genital hiatus (gh) and perineal body (pb) are also recorded. A detailed assessment is performed to determine the extent of pelvic organ prolapse.
| Degree | Description |
|---|---|
| 0 | No prolapse. Points Aa, Ap, Ba, Bp are all at –3 cm. Points C and D lie between the total vaginal length (TVL) and TVL – 2 cm. That is, C or D < TVL – 2 cm. |
| I | The most distal part of the prolapse is within 1 cm above the hymenal plane. That is, measurement < –1 cm. |
| II | The most distal part of the prolapse is within 1 cm beyond the hymenal plane. That is, measurement ≥ –1 cm but ≤ +1 cm. |
| III | The most distal part of the prolapse extends more than 1 cm beyond the hymenal plane but does not exceed the total vaginal length. That is, measurement > +1 cm but < TVL. |
| IV | Complete vaginal eversion. The most distal part of the prolapse equals or exceeds the total vaginal length. That is, measurement ≥ TVL or TVL + 2 cm. |
II Pelvic floor muscle pressure screening
The pelvic floor pressure tester can measure pelvic and abdominal pressure indicators (dynamic vaginal pressure greater than 80-150 cm water column). The pelvic floor muscle strength can be tested with a pressure balloon.
From the perspective of pelvic floor muscle type, the pelvic floor muscles are mainly composed of class I muscles and class II muscles .
Class I muscles are long-lasting muscles. During training, the pelvic floor is generally contracted for 5 seconds and relaxed for 5 seconds, which constitutes a set. 70% of the pelvic floor muscles are composed of Class I muscles; Class II muscles are fast-twitch muscles. During training, the maximum force is contracted for 2 seconds, and then relaxed for two seconds, which is repeated 5 times in a row, which constitutes a set. 30% of the pelvic floor muscles are composed of Class II muscles.
5 exercises to strengthen your pelvic floor muscles
Ⅰ Kegel exercises
Kegel exercises are exercises that contract and relax the pelvic floor muscles. If you experience urinary incontinence after childbirth, this indicates a clear sign of relaxation, and they are a necessary practice.

Main muscles worked: Pelvic floor muscles
▼Equipment required: Breathing audio
▼Specific method:
1) Use the right muscles. The simplest way to stop urinating is to use the right muscles, which are the pelvic floor muscles.
2) Contract your pelvic floor muscles and hold for 5 seconds, then release for 5 seconds.
3) Repeat 10 times, 3 times a day.
II. Pelvic rotation
Pelvic rotations use the pelvic joints and lower abdominal muscles and can cause significant muscle changes. When performing pelvic rotations, you want to ensure that you are only engaging the correct muscles and not compensating.
▼Main muscles: hip muscles, psoas muscles, gluteal muscles, etc.
▼Position: supine position with knees bent or other
▼Specific method:
1) Lie supine with knees bent (you can place a block between your knees to stabilize your lower limbs and strengthen your thigh adductor muscles), with your feet pelvis-width apart and your toes pointing parallel.
2) Left hip up, right hip down, left hip down, right hip up, pubic symphysis up, down to navel, pubic symphysis down, up to navel as if your pelvis is swinging like a round clock.
3) Strengthening training: Raise your hips 1cm and tilt left and right.
4) Repeat 15 times.
Ⅲ Hip Bridge
The glute bridge is a very effective exercise that also activates the pelvic floor muscles.
▼Major muscles: Hamstrings, pelvic floor
▼ Equipment required: Yoga brick or no
▼Specific method:
1) Lie on the floor. Your spine should be flat on the ground, knees bent at a 90-degree angle, feet flat, arms straight, palms facing down.
2) Inhale and push through your heels into your glutes, hamstrings, and pelvic floor, lifting your hips off the floor. Your upper back and shoulders should now form a straight line from your knees.
3) Pause at the top for 1-2 seconds, then return to the starting position.
4) Complete each rep in 10-15 seconds, do 2-3 times, and rest for 30 seconds.
5) If you want to make the hip bridge more difficult, you can place your feet on the ball in the starting position, lie flat on your back on the ground, and repeat the above steps.
IV. Split Leg Exercise
This is primarily a leg exercise and is the foundation for many movements in Pilates. By adding leg movement, you can also activate your hips and pelvic floor muscles.

▼Main muscles: lower abdominal muscles, pelvic floor muscles
▼Equipment needed: mat
▼Specific method:
1) With the platform on the floor, bend your knees so your thighs are perpendicular to the floor and your shins are parallel to the floor. Bring your abs up to activate your inner thigh muscles.
2) During the exercise, focus on controlling your movements and slowly separate your legs, allowing your knees to drop outwards into a comfortable position.
3) Repeat this movement slowly, 10 to 15 times each time, for a total of 3 sets.
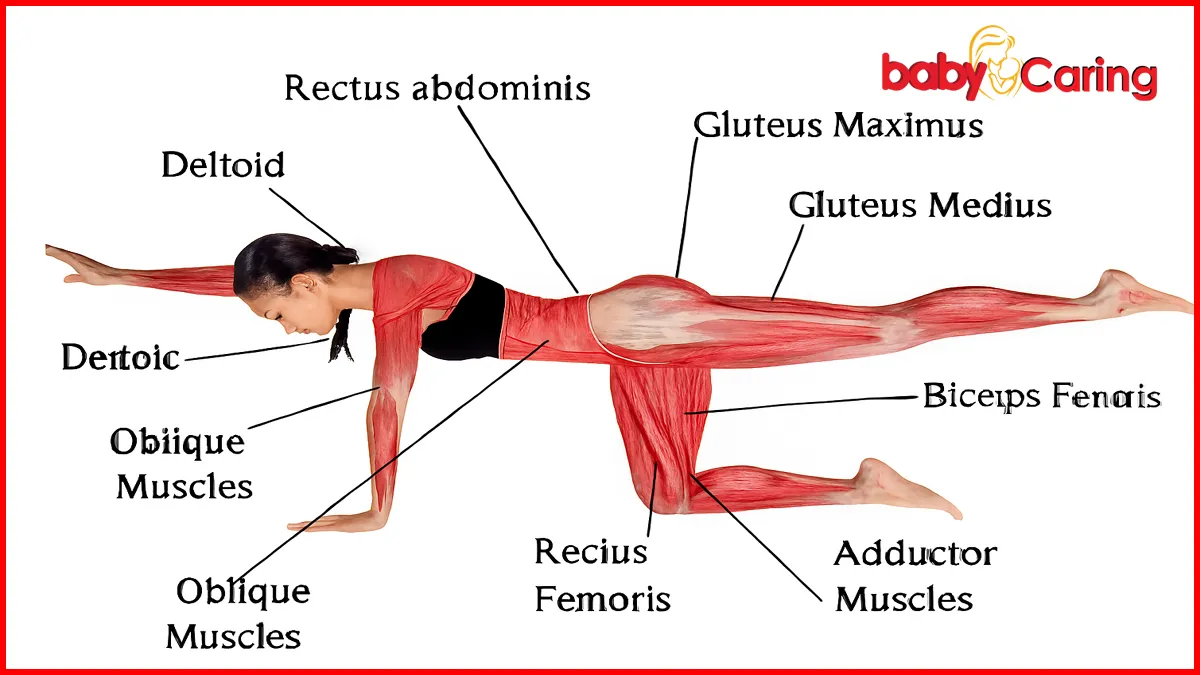
ⅤQuadrupedal Swimming
▼Specific method:
1) To begin, straighten and lift your left leg and right arm simultaneously, keeping your pelvis and shoulders in a neutral position. Do not raise or lower your head. Hold for 2 seconds.
2) Bend and lower your left leg and right arm back to the starting position while maintaining stability, then switch, raising your right leg and left arm.
3) Repeat these two movements 10 times, doing 3 sets at a time.
Wisdomom is a team of obstetricians and nurses , along with experienced maternity educators. We specialize in prenatal exercise planning and provide guidance on nutrition, emotional well-being, prenatal care, and natural childbirth. We aim to help a new generation of expectant parents improve the quality of their pregnancies, ensuring the healthy growth of their newborns and the fulfillment of their families.







